



Imagine your thoughts buried beneath layers of muck and debris.
Struggles with Recalling Specific Names Are Common in Midlife
One evening on a Friday, while my spouse and I debated dinner options, our exchange unfolded in this familiar pattern:
I asked: “Would you like to try that particular eatery?”
He replied: “Which one?”
I struggled: “The name escapes me right now. We’ve dined there previously. Remember the spot with peanut shells scattered across the floor? It’s located beside… you know the place. It’s along the street where we used to bring our dog for veterinary checkups. Does that ring a bell?”
It felt like key pieces of information were trapped in a thick, murky sludge deep within my mind’s hidden corners. Then, much later, perhaps hours afterward, the recollection would surface abruptly, prompting me to exclaim to no one in particular…
“Texas Roadhouse!”
This kind of sluggishness, especially with proper nouns like names of places, people, books, or films, is quite standard for individuals in their middle years and older.
Yet, what I was encountering more and more frequently during my late forties and into my early fifties seemed anything but ordinary.
Not just the perpetual struggle to recall names of restaurants, acquaintances, publications, films, and countless other items, but my cognitive faculties were faltering even during professional hours.
I’d position myself before my computer display, gaze blankly at an open file, and attempt to compel my fingers to produce something worthwhile. A pervasive fog enveloped everything, reminiscent of those initial groggy instants upon waking when you’ve silenced the alarm but remain too drowsy for simple calculations.
I experienced brighter periods, typically in the early hours, squeezing what I could of an eight-hour workload into the fleeting two or three hours of sharp mental acuity available to me.
On the Most Challenging Days, a Persistent Mental Cloud Lingered Unshaken
Productivity at work became impossible from the outset. I lacked the mental capacity for reading or engaging in any substantial activities.
Consulting Medical Experts for Guidance
Three different medical practitioners suggested antidepressants as the solution. I experimented with one, only to feel even more debilitated. Another followed, then a third at an elevated dosage. Regardless, I resembled a lifeless automaton. One provider prescribed a sleep aid, which intensified my drugged sensation.
Thyroid function was evaluated-perfectly normal. No signs of anemia either. I sampled various supplements, mushroom-infused coffee, and nearly every item promising enhanced cognition in its marketing.
After almost two years cycling through an array of physicians, I scheduled my routine annual gynecological examination. Casually noting vaginal dryness prompted her to probe further with inquiries unrelated to that issue: quality of sleep? Emotional state? Vitality levels? Any hot flashes? What about cognitive haze?
“It’s ironic you bring up brain fog,” I responded in my characteristic dull, foggy tone. “I feel scarcely alive.”
By the session’s conclusion, clarity emerged: depression had likely never been the culprit.
The Reality Was Menopause-Related Changes
My gynecologist provided prescriptions for estradiol and progesterone upon my departure.
Almost immediately, it was like a light switch activating in my brain.
Clear thinking returned. Typing flowed effortlessly once more. I could track discussions without losing the thread. Work extended beyond midday.
And, after years, uninterrupted sleep stretched beyond a mere two hours.
Menopause Represents a Natural Life Transition, Not an Illness
Menopause does not qualify as a pathological condition or disease.
Rather, akin to puberty, it marks a distinct phase of life-a precise shift from one reproductive stage to another.
Menopause is officially attained after 12 continuous months without menstrual bleeding. From that point, the postmenopausal phase begins.
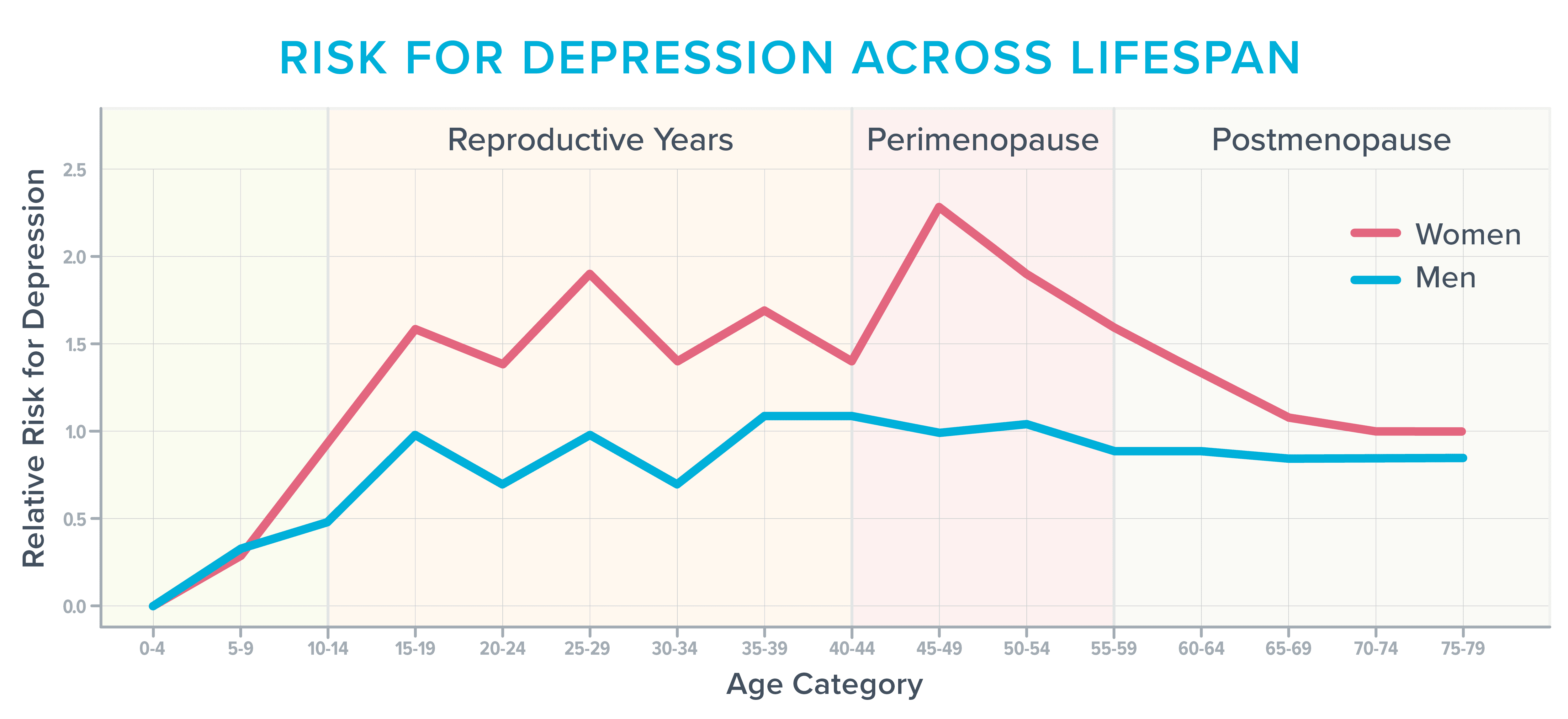
As women near this pivotal shift, their hormone concentrations oscillate and decline, sparking a wide array of symptoms. Issues like unwanted weight increase and diminished libido often dominate discussions.
Nevertheless, approximately 40 percent of women navigating perimenopause and postmenopause describe heightened irritability, emotional volatility, anxious feelings, exhaustion, and difficulties with focus, per insights from the American College of Obstetricians and Gynecologists. Meanwhile, data illustrates this period as particularly susceptible to depression onset, especially for those with prior history.
Prior to hormone initiation, unprovoked tears would overwhelm me. At other times, ordinary environmental inputs felt overwhelmingly intense.
Everyday noises-such as vehicular hum or mall chatter-physically pained my senses. I became startlingly reactive, short-tempered, and worried over formerly trivial concerns like traversing bridges or navigating roadwork zones.
Factors Driving Cognitive and Mood Disruptions Remain Multifaceted
The precise mechanisms behind these mental and emotional manifestations aren’t fully elucidated.
Hormonal fluctuations undoubtedly contribute, alongside standard brain alterations associated with advancing age.
Moreover, women in this life stage frequently juggle multiple demands that rapidly deplete mental reserves, much like a voracious entity sapping vital essence.
In their forties and fifties, many hit career pinnacles with obligations spilling into personal time, fueling sleepless worry. They might manage moody adolescents, support elderly relatives, adapt to quieter homes post-children’s departure, reassess partnerships, or grapple with escalating educational or medical financial burdens.
Yet, a subtler, under-discussed catalyst for mental unease stems directly from the iconic menopausal hallmark: hot flashes.
Understanding the Physiology of Hot Flashes
Daytime hot flashes and nocturnal sweats collectively comprise vasomotor symptoms. The term “vasomotor” pertains to blood vessel constriction or expansion, which impacts sweating, blood pressure, and more.
In a hot flash or night sweat episode, norepinephrine and cortisol surge. Vessels widen to dissipate excess heat, elevating blood pressure and pulse.
Severity varies: skin may flush as heat radiates across face, neck, and torso. Sweating, palpitations, anxiety, weariness, or dizziness might ensue.
The origins of hot flashes around menopause remain somewhat mysterious.
One prevailing hypothesis posits that declining estrogen disrupts the hypothalamus, the brain’s temperature control center. This miscalibrates the body’s thermostat, prompting erroneous overheating or overcooling signals.
Impacts of Vasomotor Symptoms on Brain Structure and Function
Historically, experts dismissed vasomotor symptoms as minor nuisances or social embarrassments.
(Truthfully, I shared that view; amid futile consultations, hot flashes never crossed my mind to disclose.)
Emerging evidence, however, indicates these episodes transcend discomfort or laundry hassles, potentially harming vascular and neural health adversely. Consequently, growing consensus views vasomotor symptoms as legitimate treatable disorders.
Hot Flashes Linked to Brain Lesions
A study involving 226 women equipped them with hot flash monitors, conducted MRIs, maintained sleep logs, and utilized smartwatches for nocturnal awakening tracking.
Analysis revealed that women with the highest hot flash frequency exhibited numerous patchy regions termed whole-brain white matter hyperintensities.
Formerly attributed to normal aging, these hyperintensities now signal heightened future cognitive deterioration risk.
Abundant lesions correlate with doubled dementia odds and tripled stroke probability.
Connections to Vascular Health
These hyperintensities may partly arise from alterations in cerebral blood supply vessels.
A longitudinal three-year examination of 492 women corroborated this, finding frequent hot flash sufferers prone to vascular impairments like poor dilation for augmented flow.
Additional studies associate recurrent hot flashes with:
- Carotid artery wall thickening supplying brain, face, and neck regions
- Elevated body fat percentages
- Rises in total and LDL cholesterol levels
- Increased insulin resistance
Disrupted Sleep as a Mediator
Beyond direct vascular effects, hot flashes indirectly impair the brain via sleep fragmentation.
Remarkably, numerous women remain unaware of hot flashes interrupting their rest.
They might attribute wakings to insomnia or apnea, as I did initially.
Night sweats don’t always involve profuse perspiration; by awakening-triggered by cortisol/norepinephrine spikes-the heat may have subsided, leaving puzzling repeated arousals.
Such disruptions hinder memory consolidation, toxin clearance, and retention of daily information like names, dates, and facts.
They also erode connectivity in the hippocampus, crucial for learning and recall.
Sleep deficits hyperactivate the amygdala, heightening emotional reactivity to stress, anxiety, irritation, frustration, or anger.
These neural shifts manifest after mere days to a week of poor sleep-consider the cumulative toll over years of fragmented nights.
Challenges in Securing Appropriate Medical Support
Depression diagnosis relies on the PHQ-9 scale: endorsing four of nine items flags depression.
Yet four items mirror menopause-induced sleep loss symptoms:
- Diminished interest or enjoyment in activities
- Difficulties initiating or maintaining sleep
- Persistent fatigue or low energy
- Concentration struggles, e.g., with reading or viewing media
Endorsing these could yield a depression label, masking underlying sleep battles commencing around age 47.
Gaps in Menopause Education for Providers
Surveys reveal 80 percent of residents feel marginally equipped for menopause discussions. Even ob-gyn programs rarely include comprehensive training.
Thus, it’s unsurprising providers overlook hot flashes or sleep issues amid complaints of lethargy, motivation deficits, and focus lapses.
Even recognizing vasomotor contributions to cognitive/emotional woes, many hesitate on menopausal hormone therapy (MHT or HRT), deeming it unsafe or hazardous.
This embodies “defensive medicine,” per menopause specialist Jerrold H. Weinberg, MD, from Michigan.
“It’s an instinctive doctor response to treatment suggestions,” Dr. Weinberg explains, “driven by litigation fears.”
Current Evidence on Hormone Therapy Safety and Efficacy
Such caution stems from dated studies associating specific hormones with marginal breast cancer or stroke risk elevations.
Contemporary analyses qualify this: risks hinge on age, dosage, formulation, and therapy duration.
For those under 60 and within 10 postmenopausal years, benefits typically surpass risks for moderate-severe symptoms, per expert consensus.
Countervailing gains include lowered Alzheimer’s and osteoporosis risks, with Dr. Weinberg affirming MHT’s net positives for most.
While select antidepressants alleviate mood, sleep, and flashes, they carry side effects. Defensive practitioners favor them as lower-risk alternatives.
Strategies for Effective Health Advocacy During Menopause
For those endlessly seeking menopause-savvy providers, heed guidance from Dr. Weinberg and Helen Kollias, PhD-physiology/molecular biology authority and science advisor at Precision Nutrition and Girls Gone Strong.
▶ Consult menopause-certified specialists.
They often highlight this expertise in profiles, noting menopause focus areas. Databases from organizations like the Menopause Society list certified practitioners.
▶ Log symptoms meticulously.
Documenting aids recall during foggy appointments and evaluates treatment efficacy, guiding dosage or alternative adjustments.
Track metrics like:
- Hot flash frequency
- Daily brain fog duration
- Incidence of fatigue, anxiety, anger, etc.
- Nocturnal awakenings count
▶ Provide precise details in consultations.
Vague “poor sleep” elicits less targeted aid than “Over seven days, only one night yielded four solid hours; averaging five wakings nightly, max stretch three hours.”
Smartwatch data showcased via app bolsters credibility.
▶ Engage in balanced treatment dialogues.
“Shared decision-making” fosters open benefit-risk talks, collaboratively tailoring choices-reducing complaints and suits, easing defensive stances.
Sample queries:
- “Could MHT suit me? Let’s explore candidacy.”
- “I’ve seen notes on breast cancer risk; can we assess mine via family history, age, BMI, habits?”
- “Familial osteoporosis/dementia concerns me; MHT’s protective potential plus sleep aid-pros/cons?”
9 Practical Lifestyle Approaches to Bolster Mental and Emotional Well-Being in Menopause
Habits enhancing psychological and emotional resilience amid menopause largely mirror universal health promoters across ages and genders.
No unique diet exists for vasomotor relief beyond curbing caffeine, alcohol, spicy/hot fare. (Soy like tofu offers limited aid despite past hype, though nutritionally sound.)
Approach 1: Prioritize Core Wellness Foundations
Midlife demands no overhaul of basics like nutrition, movement, stress mitigation, recovery, connections, purpose-yet adherence grows paramount.
Self-assess:
- Sufficient sleep/rest allocation?
- Consistent physical engagement?
- Nutrient-dense intake: vibrant produce, quality fats, proteins, fibers, legumes?
- Meaningful social interactions buffering stress?
- Experiences fostering wonder, delight, inquisitiveness, serenity, meaning?
Negative responses warrant barrier analysis: what’s impeding? How to dismantle obstacles or enlist aid?
Approach 2: Incorporate Creatine Supplementation Trials
Beyond preserving muscle/bone amid age/hormonal shifts, creatine supports mood, cognition, fatigue resistance-even offsetting sleep deficits. Studies endorse 5-7g daily creatine monohydrate.
Approach 3: Establish Routine Sunlight Exposure
Sunlight boosts alertness, synchronizes circadian rhythms for evening drowsiness/morning vigor-morning/late-afternoon optimal.
Among 103 participants, a.m. outdoor time forecasted superior sleep: faster onset, extended duration, fewer disruptions.
It additionally elevates mood/focus.
Approach 4: Moderate Gym Intensity Judiciously
Exhaustion plus prolonged high-intensity bouts exacerbate fatigue.
Midlife injury susceptibility rises; recovery prolongs versus youth.
Overloading yields soreness, irritability, tension, exhaustion.
Conversely, brief exertions mimic invigorating cold plunges for daytime alertness.
Desk drowsing? Opt for 5-10min walks, pushups, squats outdoors.
Pre-bed gentle pursuits like yoga/stretching promote unwind-avoid intensity triggering adrenaline.
Attune to bodily feedback, particularly post-poor sleep.
Vigorous efforts/PBs viable occasionally; modulate via sleep/recovery: swap runs for zone 2 cardio, trim resistance sets/reps/loads.
Balance intensity with moderation/recovery dynamically.
Approach 5: Explore CBT-I for Sleep Optimization
Cognitive Behavioral Therapy for Insomnia equips reframing skills for robust sleep hygiene, e.g., fixed wake times irrespective of prior night.
Approach 6: Confront Stress Realistically
Midlife energy may not match youth’s boundless checklists.
Audit time/energy logs critically: align with priorities? Permit self-care/recovery, or others-dominated?
Modifications for rest? Coaches: deploy stress wheels pinpointing drains for targeted relief. Boundaries via “no” foster self-prioritization.
Approach 7: Trial Cooling Aids for Sleep
Cooler ambiances curb sweats/enhance rest: lower thermostat, fans, chilled mattress overlays.
Approach 8: Embrace Strategic Pauses
Foggy productivity futile-sanction 20min idles: iced drinks, pet snuggles, window gazing, nature sounds, friend chats.
Quick reset: 5min body scan. Comfortable pose (legs-up-wall, knee-pillowed supine). Eyes shut, sensation-sweep head-to-toe; neutrally observe. Note post-scan: physical/emotional states? Thoughts?
Approach 9: Adopt Circulation-Supportive Eating Patterns
Cardio-protective foods safeguard cerebral vessels too.
MIND/Mediterranean styles-veggie/fruit/whole grain/olive/bean/fish-rich-lower Alzheimer’s/depression risks.
Nitrate sources (beets, greens) vasodilate, transiently boosting cerebral bloodflow/memory.


